Lower Limb Salvage, successful Aorta bifemoral bypass via left retroperitoneal approach combined with regional anaesthesia.
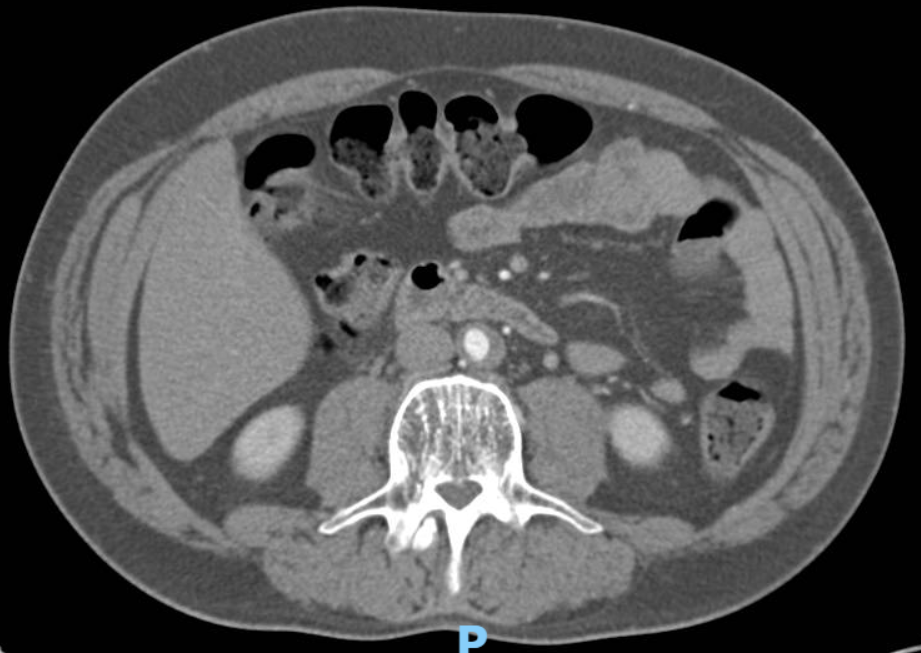
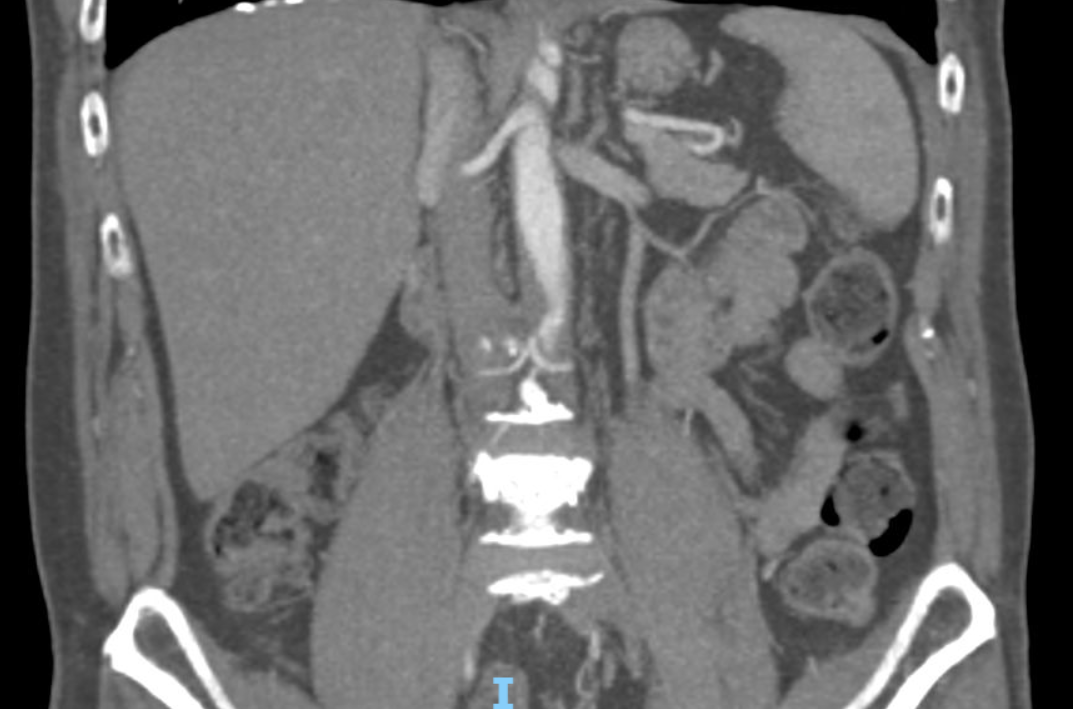
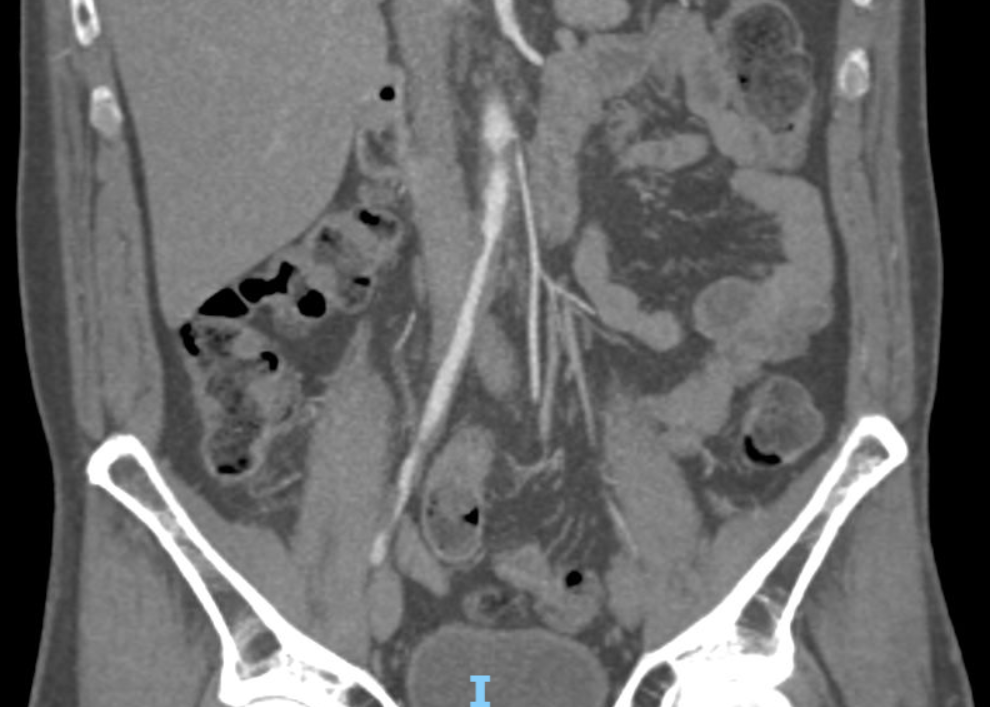
54 years old male, Over last 2 – 3 weeks he developed on his left foot change in his temperature coolness, rest pain and blue discolouration on his left 5th toe, was admitted from A&E without evidence of bilateral femoral pulses.
He is active smoker, 10 – 15 cigarette per day; Asthma; Osteoarthritis; CVA Stroke; Right Frontal lobe infarct; 60% Left ICA stenosis; Long history 10 year ago of back pain with several infiltration on his Sacro-iliac joint; Severe lumbar vertebral canal stenosis with caudal equina compression; Long history of bilateral lower limb intermittent claudication around 200 yards.






Surgical Technique:
The procedure was carried out in a full equipped operation suite under general and regional anesthesia - spine.
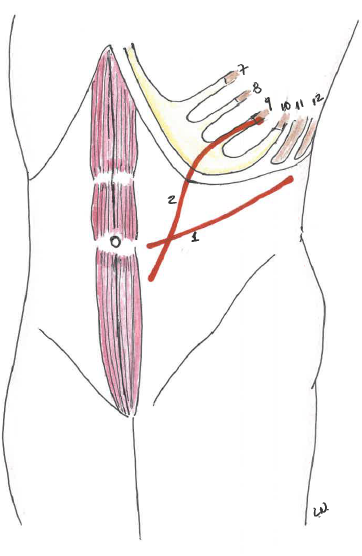
The patient was positioned on a bean-bag device with the left shoulder rotated superiorly and to the right by 45° and the left pelvis angled slightly. The operating table was fully broken head down to increase the space between the costal margin and iliac crest. We used a right Rob incision begun at lateral edge of the rectus abdominis approximately 2 cm below at umbilicus and it extended curvilinearly toward the superior margin of the 11th, 12th rib.
The latissimus dorsi, intercostal, external oblique, internal oblique, and transversalis muscles are divided using electrocautery. The peritoneum was then reflected medially off Gerota's fascia exposing the retro-peritoneum, the dissection proceeds medially and anterior to the psoas muscle and ureter.
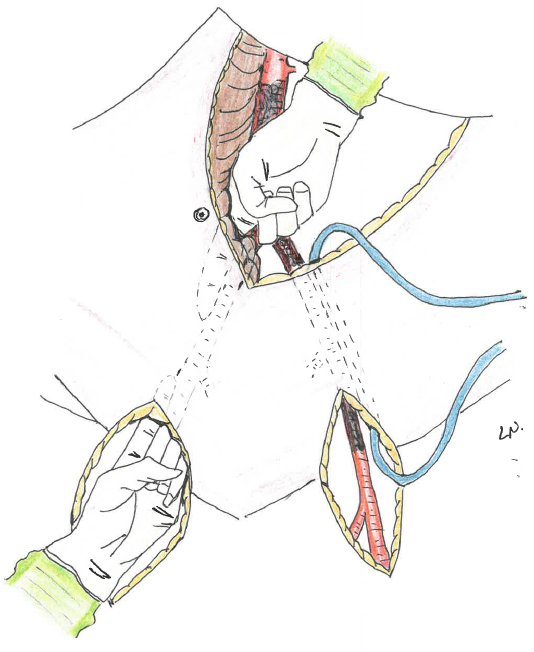
A tunnel for the right branch graft is created, gentle dissection, from the right common femoral artery and from the right common iliac artery, with the index or middle finger of each hand following the anterior surface of the iliac artery, avoiding venous injuries, intestine and ureter,


Post - Operator:
Extubated immediately after surgery, hemodynamic stability without need for catecholamine therapy, recovery observation for 4 hours, transferred to ward, discharge 5 days after.
In 1963, Rob was the first to give a detailed description of the antero-lateral retroperitoneal approach. In 1980, Williams et al. described the extended retroperitoneal approach, which allows a better exposure not only of the infrarenal but also the pararenal and even suprarenal aorta.
Charles Granville Rob MC FRCS (4 May 1913 in Weybridge, England. – 26 July 2001 NY) was a British surgeon.
Rob C. Extraperitoneal approach to the abdominal aorta. Surgery 1963;53:87-89.; Shumacker HB. Midline exposure of the abdominal aorta and iliac arteries. Surg Gynecol Obstet 1972;135:791-792.
George Melville Williams, M.D. (1930 China in Soochow, China - August 26, 2020, of complications of novel coronavirus disease-19 infection in Stuart, Florida) was an US surgeon.
Williams GM, Ricotta J, Zinner M, et al. The extended retroperitoneal approach for treatment of extensive atherosclerosis of the aorta and renal vessels. Surgery 1980; 88:846-855.